



Health interventions typically favour pregnant women and children under 5 years of age. A prism that does not take into account other ever-growing vulnerable populations: the indigents and the elderly. The authors demonstrate here how the proper use of tools and demographic data would provide more relevant targeting.
Not a day goes by without public health experts and the World Health Organisation (WHO) referring to the need to reform public health systems in order to move towards Universal Health Coverage (UHC) and “leave no one behind”[1]Following the watchword “Leaving No One Behind”, the cornerstone of the United Nations’ 2030 Sustainable Development Agenda, presented in 2015.. In addition to their advocacy work[2]See Oxfam, for example, and its report entitled «Idées reçues sur la gratuité des soins» , published in French and English: https://journals.openedition.org/factsreports/1723), implement reference-evacuation systems, improve the quality of care, and support community health workers (Muso in Mali). But still too often, and especially in West Africa, NGOs tend to focus on target populations, referred to as “vulnerable populations” in public policy, which include pregnant women and children under five. The global vision of these target populations seems to drive aid workers, without calling into question the existence of sub-groups within these populations.
NGOs must act in favour of the indigents and the elderly
The fairness of interventions is therefore a central concern, and the question of effectiveness cannot monopolise all efforts, even though certain NGOs believe that care for the indigents should fall within the remit of the State. Hence, NGOs (and therefore, naturally, their sponsors) often implicitly neglect the most vulnerable amongst the vulnerable, those that the political decision-makers of Africa still refer to as indigents. The 1990s acknowledgement of the absence of action in their favour[3]Miloud Kaddar, Friedeger Stierle, Bergis Schmidt-Ehry, Anastase Tchicaya, «L’accès des indigents aux soins de santé en Afrique subsaharienne», Revue Tiers Monde, n°164, 2000, p.903‑925. is still valid 30 years later. Moreover, the proportion of elderly people over 60 in Africa is constantly rising and is set to double by 2050[4]Nicole Atchessi, Valéry Ridde, Seye Abimbola, María-Victoria Zunzunegui, “Factors associated with the healthcare-seeking behaviour of older people in Nigeria”, Archives of Gerontology and … Continue reading. We are in the midst of a societal transformation, a subject for population science if ever there was one. Our work in Burkina Faso shows that indigents, as defined by rural communities, are overwhelmingly elderly people, often widows[5]Samiratou Ouédraogo, Valéry Ridde, Nicole Atchessi, Aurélia Souares, Jean-Louis Koulidiati, Quentin Stoeffler et al., “Characterisation of the rural indigent population in Burkina Faso: a … Continue reading. These people live in extremely difficult conditions, often socially and geographically isolated, and only rarely benefit from public policies and NGO projects[6]Kadidiatou Kadio, Aboubacar Ouedrago, Yamba Kafando, Valéry Ridde,«Émergence et formulation d’un programme de solidarité pour affilier les plus pauvres à une assurance maladie au Burkina … Continue reading. Naturally, it is not easy to take them into account, but the tools and science of demographics could be valuable in terms of identifying and understanding these populations, who are amongst the neediest. Population science makes it possible to highlight the perennial nature of these situations of extreme poverty, and the increasing demographic weight of the elderly, as shown by the Population Observatory in Ouagadougou[7]Yentéma Onadja, Sara Randall, Vincent Léger, «Santé et bien-être des personnes âgées: appréciation qualitative et approche par les limitations fonctionnelles», inClémentine Rossier, … Continue reading. Intergenerational solidarity with the elderly in Burkina Faso is rapidly changing and their health care needs are not being taken into account.
Indigents and elderly people in the context of current UHC policies
Using these demographic tools could certainly strengthen policies in West Africa which have finally, unlike NGOs, begun to take an interest in indigent and elderly people. Mali, Burkina Faso and Senegal offer three interesting contemporary examples to illustrate the relevance of this reflection[8]Since 2010, Uganda has been organising a money transfer programme for elderly people, which benefited over 150,000 people in 2017.. In the context of actions to be undertaken for UHC, Mali has committed to an ambitious policy to provide free access to care for the indigents, using only national funding[9]Céline Deville, Fatoumata Hane, Valéry Ridde, Laurence Touré, «La Couverture universelle en santé au Sahel: la situation au Mali et au Sénégal en 2018», working paperdu Ceped, n°40, Ceped … Continue reading. The “Régime d’assistance médicale” (RAMed) was launched in 2011. Its goal is to register people and offer a free health care package to the 5% of the population considered to be the poorest. We do not know how this figure of 5% was arrived at, and the issue of the definition of indigence and the selection criteria remains. Registration is essentially carried out by social services, but given the challenge of its organisation on a national scale, the role of NGOs and community organisations is increasingly highlighted. This is especially true given that the World Bank offers incentives to a number of countries in the region to set up Unified Social Registers (USR), including the names of all those selected to benefit from social programmes. In Mali, this USR has a list of more than 200,000 indigents associated with RAMed, but also a list of beneficiaries of social safety net programmes (71,000) and programmes by NGOs such as Action Contre la Faim (3,500) and Solidarités International (1,700).
In 2012, in Burkina Faso, the State decided to launch a pilot solidarity programme to reinforce access to care for indigents by means of mutuelles. These mutuelles are often seen as tools for UHC, but we know that the poorest cannot afford to subscribe to them. This programme was to enable indigents to subscribe to mutuelles for free. Nevertheless, this coverage in the country remains very low, the budget allocated is insufficient (4,500 beneficiaries), health workers’ interest is minimal, and the content of the programme was not developed according to the needs of the indigents (especially with regard to the service package offered and the retaining of a co-payment)[10]Kadidiatou Kadio, Kafando Yamba, Ouédraogo Aboubacar, Valéry Ridde, “Analysis of the implementation of a social protection initiative to admit the poorest of the poor to mutual health funds in … Continue reading. In 2015, the law on universal health insurance decreed that indigents would receive it free of charge and that the State would cover their subscription costs. Nevertheless, unlike in Mali and in Senegal, the selection and registration process for these indigents is struggling to get off the ground, in spite of the experiences which we will see in the next section.
Senegal also developed such policies for indigents, but also, unusually for the region, for the elderly. For the indigents, the country decided to follow the example of Rwanda, giving free subscriptions to mutuelles, which cover most of the country. These people also receive national family welfare grants (FWG) which allow them to receive money transfers. The initial aim was to reach 300,000 beneficiaries. For the elderly, since 2006, the Sésame plan has targeted people over 60 in order to give them access to free health care. It is currently experiencing financial and implementation difficulties, which have reduced its effectiveness[11]Ousseynou Kâ, El Hadji Mbaye, Mamadou Makhtar Mbacké Leye, Atoumane Faye, Alioune Badara Tall, Awa Gaye et al., « Plan Sésame au Sénégal: limites de ce modèle de gratuité », Santé Publique, … Continue reading.
This overview of the policies of three West African countries in favour of indigent and/or elderly people shows the extent to which the definition of their content, and especially their implementation, remain problematic. For now, it is less a financial issue than a formulation challenge. To account for these challenges, we will set out the specific case of Burkina Faso, because we have been carrying out research on indigence there for 15 years and the context is interesting to share for other countries and NGOs to learn from it.
Community selection and indigence in Burkina Faso
For elderly people, definitions vary depending on the organisation or continent (over 60 years old according to the United Nations, over 50 for low-income countries, according to the WHO), but they remain relatively clear since the threshold value is age. But for indigents, the definition is more complicated. Who is indigent? According to which criteria? Mali decided, without in-depth study, that the indigents were the poorest 5% of the population, whereas Burkina Faso has yet to decide on a proportion, even though 9% of its population live under the extreme poverty line.
After several pilot research-action projects begun in 2007 to find a socially acceptable process to fairly and effective select indigents to benefit from free care, Burkina Faso launched a wide-reaching intervention in 2015, on a scale of more than 1.7 million people. It was carried out in the context of a World Bank-funded health system reform (performance-based financing). In nearly 1,200 villages, local committees rallied around a consensual definition of the concept of an indigent – “someone who is extremely disadvantaged socially and economically, unable to look after himself (herself) and devoid of internal or external resources”. They then selected those people whom the villagers believed should benefit from a card granting free access to primary health care.
The selection process and exemption from payment were entirely funded by the World Bank programme. More than 6% of the population (102,609 people) were considered to be indigent by the communities, demonstrating that it is possible to organise a community targeting process on a large scale. This coverage did, however, vary considerably from one district to another, between 3% and 19%. On the other hand, the process was very expensive, its financial and economic (including the value of volunteer time) costs are respectively estimated at $5.7 and $11.83 per person selected[12]Yvonne Beaugé, Jean-Louis Koulidiati, Valéry Ridde, Paul Jacob Robyn, Manuela De Allegri, “How much does community-based targeting of the ultra-poor in the health sector cost? Novel evidence from … Continue reading. But how to find a cheaper community selection solution? Moreover, it was not possible to calculate the cost-effectiveness relationship of this process because it simply was not effective from the point of view of the indigents. A quarter of indigents never received their card, demonstrating the challenges relating to implementation. Above all, those who were sick and in possession of this card in 2017 were not able to benefit from it, as the experience in 2007 had shown[13]Nicole Atchessi, Valéry Ridde, María-Victoria Zunzunegui, “User fees exemptions alone are not enough to increase indigent use of healthcare services”, Health Policy and Planning,2016 Jun;31(5), … Continue reading. In 2019, a cohort study of the same population showed that the average number of use of care to care by indigents who had received a card since 2017 was only 2.1 in two years.
NGOs and non-financial factors in access to care
These disappointing results are not surprising, since they confirm the challenges that are widely referred to in terms of improving fairness in access to care and “leaving no one behind”. But these studies should not become a pretext for inaction and immobilism. NGOs must be able to take part in the search for operational solutions and give themselves the means to evaluate the effectiveness and processes of these solutions. A number of operational issues remain. When we consider the barriers to accessing health services (Figure 1), we can clearly see that the issue of paying for care is but a drop in the ocean of problems for indigents. This financial barrier remains very significant, but unlike pregnant women and children, who benefit very widely and quickly from the direct payment exemption, indigents face a host of other, more pervasive obstacles.

Source: © 2013 Levesque et al.[14]Jean-Frédéric Levesque, Mark F. Harris, Grant Russell, “Patient-centred access to health care: conceptualising access at the interface of health systems and populations”, International Journal … Continue reading licensee BioMed Central Ltd.
The indigents selected by these community processes often live relatively close to health centres and local officials. In spite of this, they do not always make sufficient use of them when they need to. How can we support those who are geographically more isolated? Taking the example of the Ouargaye District in Burkina Faso (Figure 2), the map shows the location of groups of people qualified as indigent by the community. The darker the colour (brown) on the map, the bigger the group. The biggest groups are to be found in proximity to health centres (red cross). Conversely, the smallest groups (yellow), made up of isolated indigents, are often the furthest removed from the health centres.

In the context of Burkina Faso, these indigents are often elderly, widowed, socially-isolated women. In addition to their material deprivation, they have significant physical and mental health issues (getting around, expressing themselves, remembering things). They have various needs which do not all fall within the remit of health care. They are not always empowered to interact with health professionnals, or to know and claim their rights. How can we support these people in their search for care and accompany them through the maze of health care, including when care is free? The concept of patient navigation is interesting to mention, and the role of NGOs turns out to be critical in experiments in this domain.
Patient navigation: a worthwhile area of intervention for NGOs
The patient navigation is a social intervention involving a person, or a group of people, who play the role of “navigator(s)” in order to facilitate access to care for people who are disconnected (marginalised, excluded) from health systems, by taking action relative to the barriers to accessing health care[15]Nancy Carter, Ruta K. Valaitis, Annie Lam, Janice Feather, Jennifer Nicholl, Laura Cleghorn, “Navigation delivery models and roles of navigators in primary care: a scoping literature review”, BMC … Continue reading. Whilst this kind of intervention seems promising, we do not know many NGOs in Africa who have committed to organising such programmes for the indigents and the elderly in the long term. At the beginning of the 2000s, in Mali, Doctors Without Borders-Luxembourg attempted to set up an assistance fund for the indigents in two district hospitals, but it did not work. The NGO gave up on the idea, as did the International Research and Development Centre (CIDR) after its experiences in Comoros and in Guinea. Also in the 2000s, in Burkina Faso, Pharmacists Without Borders (PSF) put aside the issue which was deemed too complicated, secondary, and risky for the achievement of the project’s aims with regard to its European sponsor. Agir and Planète Enfants & Développements et up support programmes for vulnerable populations (less than 1000) living in informal settlements in Ouagadougou at the end of the 2000s.
Yet significant needs remain for these people, and NGOs possess an undeniable capacity for social innovation (see example of Partners in Health, box below).
| Partners In Health
Partners in Health (PIH) has led navigation programmes for a number of years, based on “accompagnateurs” in several low-income countries such as Rwanda, Liberia, Malawi and Haiti. In Rwanda, PIH set up a community support programme, in partnership with the Ministry of Health. It involved daily house visits to HIV-positive patients by community health workers (CHWs), in order to reduce barriers to the access and adherence to antiretroviral treatment. A mobile team carried out screenings amongst the communities. CHWs offered to accompany HIV-positive patients to information and support groups. The patients received transportation allowances to attend these groups. CHW’s supply social support, monitored the side effects of treatment, identified potential obstacles to adherence and directly observed ingestion of medications. The patients therefore received support throughout their care pathways, from diagnosis to follow-up care[16]Michael L. Rich, Ann Miller, Peter Niyigena et al., “Excellent clinical outcomes and high retention in care among adults in a community-based HIV treatment program in rural Rwanda”, Journal of … Continue reading. |
We carried out a scoping review of the scientific literature on navigation experiences acting on at least two barriers to access to care and linked to people’s abilities (Figure 1) in low-income countries. We were only able to find 48 interventions in the databases. No navigation experience in Africa in favour of indigents was identified. The main targets of these interventions (73%) are people with HIV, pregnant women and children (Figure 3), but never indigent or elderly people. This is an alarming finding, but also one that might galvanise NGOs.

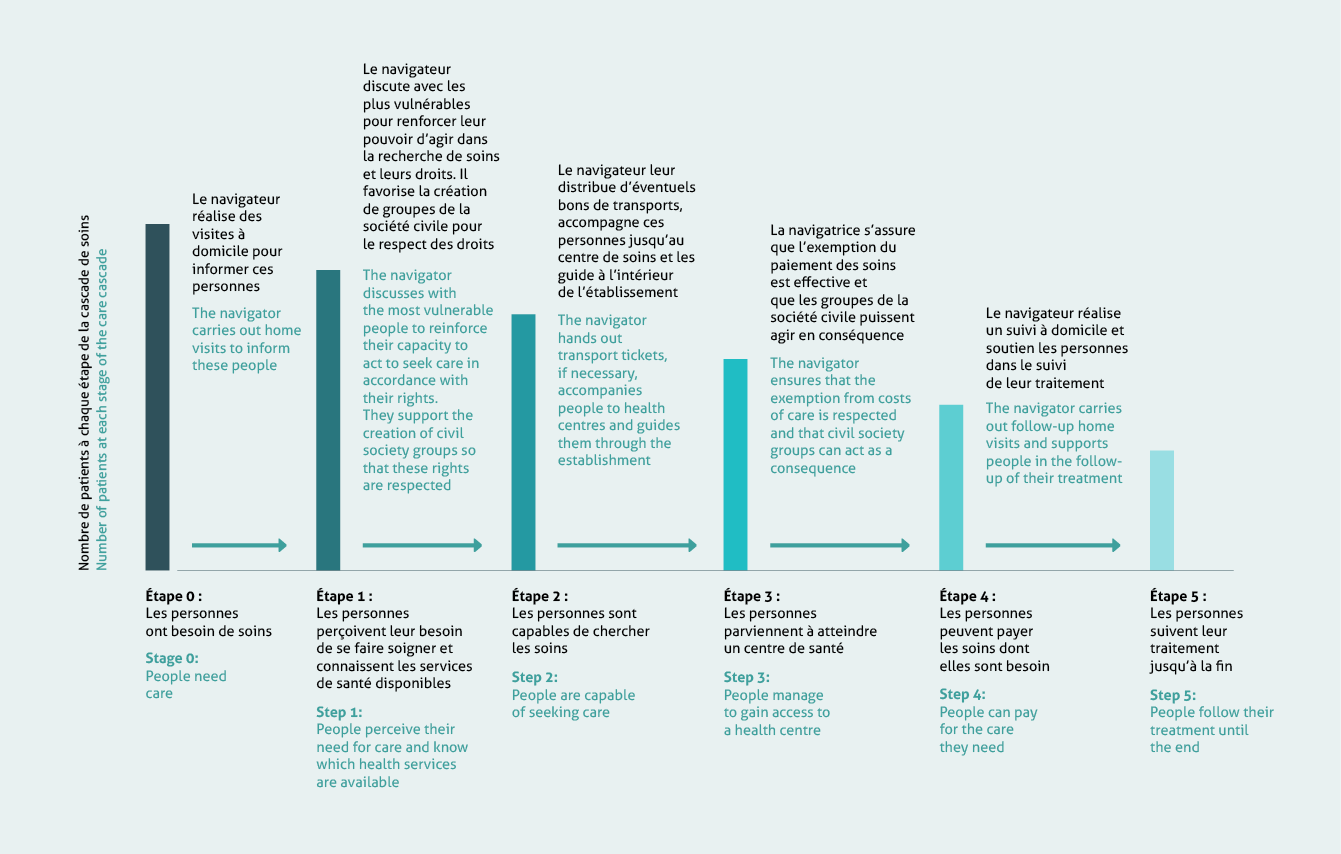
Nevertheless, it seems necessary to develop and organise interventions to accompany the most vulnerable people throughout their care pathways. Indeed, there is a very significant disparity between the number of people requiring care and the number who actually receive it, even when the care is free. Several possible courses of action could reduce this disparity (Figure 4).
Naturally, we do not have answers to every question, and we cannot give turnkey solutions. It seems to us that it is essential for NGOs, as actors of social change, to play an active role in the implementation (research-action) of such innovative interventions in order to produce evidence to inform decision-makers in West Africa for the benefit of indigent and/or elderly people. UHC ought not benefit (nearly) everybody except the indigents and the elderly. There is an urgent ethical imperative to find a solution to this demographic issue.
Translated from the French by Juliet Powys
| ISBN of the article (HTML) : 978-2-37704-582-2 |



