
Where do epidemics come from, how do they spread, and how do they behave? To answer these questions, and to introduce this issue’s theme, it was first deemed necessary to consider Covid-19’s place in the long line of previous epidemics and develop a better understanding of those yet to come. Jean Freney has risen superbly to the challenge.The recent outbreaks of H1N1 swine flu, H5N1 avian flu, the coronavirus responsible for severe acute respiratory syndrome (SARS), the Ebola virus in Africa, and now Covid-19, are a strong reminder of our vulnerability to new threats to human health and of our current inability to predict or prevent such events.
For 99% of his existence, man has been a hunter-gatherer. It is estimated that the population of the world was around one million hominids 300,000 years ago, three million 25,000 years BCE, five million just before the agricultural revolution 12,000 years ago, and 300 million at the beginning of the CE. It currently stands at around 7.5 billion individuals[1]Norbert Gualde, Comprendre les épidémies. La coévolution des microbes et des hommes, Paris, Le Seuil, 2006..
Between 200,000 and 15,000 years BCE, the human species spread across the globe followed by a cortege of parasites, viruses and bacteria. The hunter-gatherers were almost certainly affected by diseases such as those caused by head and body lice (scrub typhus, relapsing fever), pinworm infections, yaws, tularaemia, leptospirosis and schistosomiasis. It is likely that the first humans became infected by consuming contaminated carcasses (toxoplasmosis, trichinosis), but also through injuries caused by animals or contact with telluric germs (tetanus). They were certainly infected by insect bites or tick bites transmitting infections such as yellow fever and dengue fever. Nevertheless, infections must have been rare, and few virulent infectious diseases were able to survive because of the size of the social groups, composed of a few dozen individuals living in low density across large areas. This situation changed very little until the agricultural revolution[2]Serge Morand, La prochaine peste. Une histoire globale des maladies infectieuses, Paris, Fayard, 2016..
A brief history of epidemics
The agricultural revolution was a major turning point in human history because the development of agriculture brought settlement and the formation of villages and then towns. It occurred between 10,000 and 2,500 BC and began on the banks of the Nile in Egypt and the Tigris and Euphrates in Mesopotamia, together forming the Fertile Crescent. It then developed independently in several parts of the globe along the great rivers such as the Ganges, the Indus and the Yellow River.
The vast majority of the main infectious diseases in temperate zones seem to have appeared in the Old World (Africa, Asia and Europe), often via microorganisms (bacteria, viruses or parasites) hosted by large domesticated mammals and which, as a result of mutation, adapted to humans and transmitted many infectious agents to them (Table 1). In South America, lamas, which lived semi-freely – unlike the domesticated animals in the Old World – seem to have been responsible for very few infections in humans[3]Serge Morand, K. Marie McIntyre, Matthew Baylis, “Domesticated Animals and Human Infectious Diseases of Zoonotic Origins: Domestication Time Matters”, Infection, Genetics and Evolution: Journal … Continue reading. Unwanted domestic animals such as rodents also multiplied and formed permanent habitats in and around dwellings. Recent advances in genetics and phylogeography have shown that some infectious agents such as the causative agent of tuberculosis, Mycobacterium tuberculosis, are much older and existed between 2.6 and 2.8 million years ago, well before the first humans[4]M. Cristina Gutierrez et al., “Ancient Origin and Gene Mosaicism of the Progenitor of Mycobacterium Tuberculosis”, PLoS pathogens, vol.1, 1, 2005.. Nevertheless, the agricultural revolution, thanks to the increasing population density and the advances in agriculture and livestock it brought, was a powerful accelerator of infectious diseases transmitted by animals, commonly known as zoonoses (Table 1).
When man was a hunter-gatherer and constantly on the move it was difficult for a mosquito to adapt to such a nomadic host, but when man started to settle, some insect species became accustomed to feeding exclusively off this new host. This is how certain species of mosquito exhibiting strict anthropophagic characteristics, such as Anopheles gambiae, the vector of malaria, and Aedes aegypti, the vector of arboviruses (yellow fever, dengue fever), evolved[5]Jean-François Saluzzo, Des hommes et des germes, Paris, PUF, 2004.. The practice of irrigation and the development of ponds and lakes increased the number of potential breeding sites for the mosquitoes that carry yellow fever and filariasis, and also allowed contact with cercariae – the larval form of parasites that live in an intermediate host – which cause urogenital bilharzia (Egyptian haematuria). The use of faecal matter as a fertiliser must also have given rise to various infections (intestinal flukes, enteropathogenic bacteria, etc.).
Table 1 – The domestication of large mammals and rodents and their role as zoonoses, based on Morand et al.[6]Serge Morand, K. Marie McIntyre, Matthew Baylis, “Domesticated Animals…”, art. cit. and Diamond[7]Jared Diamond, Guns, Germs, and Steel: the Fates of Human Societies, New York, Norton, 1997.

Substantial population growth in the Middle East and Asia fostered infections produced by viruses (rubella, measles, mumps, chickenpox, etc.) that do not have an animal reservoir – these are the mass contagious diseases (“crowd diseases”). They emerged locally in the form of brief outbreaks. These diseases could only survive in dense populations, which was possible in the large human concentrations found in Mesopotamia, Egypt and Asia. For a virus to persist, it needs a population group of between 250,000 and 500,000 people and the ability to constantly encounter unprotected individuals (newborns and young children) at a rate of 40,000 per year.
The Spanish Conquistadors enjoyed, so to speak, a “decisive advantage” when they set out to conquer the New World in the late 15th century: not only were they protected against many infections acquired in childhood (measles, smallpox, etc.), but they also brought germs that were unfamiliar to pre-Columbian populations, which contributed to their weakening or even demise.
Two hundred years ago, most people never moved more than 30 km away from their birthplace. This meant that diseases tended to move slowly and generally within a specific climatic zone. Today, however, now that globalisation has turned the Earth into a village and mass travel has developed, the patterns of disease migration have changed dramatically. Combined with climate change, pathogens have spread far from the areas where they were born, to the extent that new infectious diseases are being described on a regular basis.
How do epidemics emerge?
For an infectious agent to cause an epidemic, it must first be able to spread rapidly from one individual to another, then encounter a sufficient number of non-immune subjects at a given time and lastly, if possible, be transmitted by aerosol means, as is the case with measles, rubella, mumps, influenza and Covid-19. The plague became a pandemic as soon as pneumonic plague appeared[8]Jean-François Saluzzo, Des hommes…, op. cit..
Now that globalisation has turned the Earth into a village and mass travel has developed, the patterns of disease migration have changed dramatically.
A pathogen can be transmitted both directly and indirectly. Direct transmission is where the infectious agent passes directly from one person to another through speech, coughing, sneezing (rhinovirus, Covid-19), food (cholera, enteropathogens), blood (HIV, hepatitis C), semen (HIV) or skin contact (herpes). Conversely, indirect transmission is where a vector (an insect or mite), an inert vehicle (food, water, objects or linen), or particles in the air carry the pathogen to the host or when its site contains an intermediate host.
The adaptation of a virus of animal origin to humans is, arguably, a rare and totally random process. In order to cross the species barrier, the virus must be released in massive quantities by the animal, adapt to humans, and eventually display the tissue tropism (cutaneous, pulmonary) required for its human-to-human transmission[9]Ibid.. This stage also requires certain adaptations allowed by the plasticity of viral genomes. Viruses multiply rapidly, and as is the case with every living being, this multiplication provides the opportunity for random changes in their genetic material because replication is not always perfect. Viruses, however, do not have genome-repair systems, as is the case for human DNA for example. These replication errors have the effect of producing mutations that at some point will make a virus present in an animal unpredictably adapt to humans[10]Mutations are also more frequent when the genetic medium is RNA rather than DNA, which is the case for coronaviruses.. Once transmitted to the host, the virus continues to evolve to its advantage or disadvantage. During the SARS outbreak, for example, the virus underwent a mutation that made it less virulent, but there is still a risk that the virus will become increasingly adapted to humans and that its virulence will increase.
From its natural reservoir – most often an animal species such as bats – the virus can be transmitted directly to humans (such as the rabies virus) or involve several host species that are then called intermediate species: SARS reached humans via the Asian palm civet found in southern China’s wet markets, MERS via camels, Ebola via gorillas and chimpanzees, Nipah via swine, the Hendra virus via horses, the Marburg virus via African green monkeys and Covid-19 perhaps via pangolins.
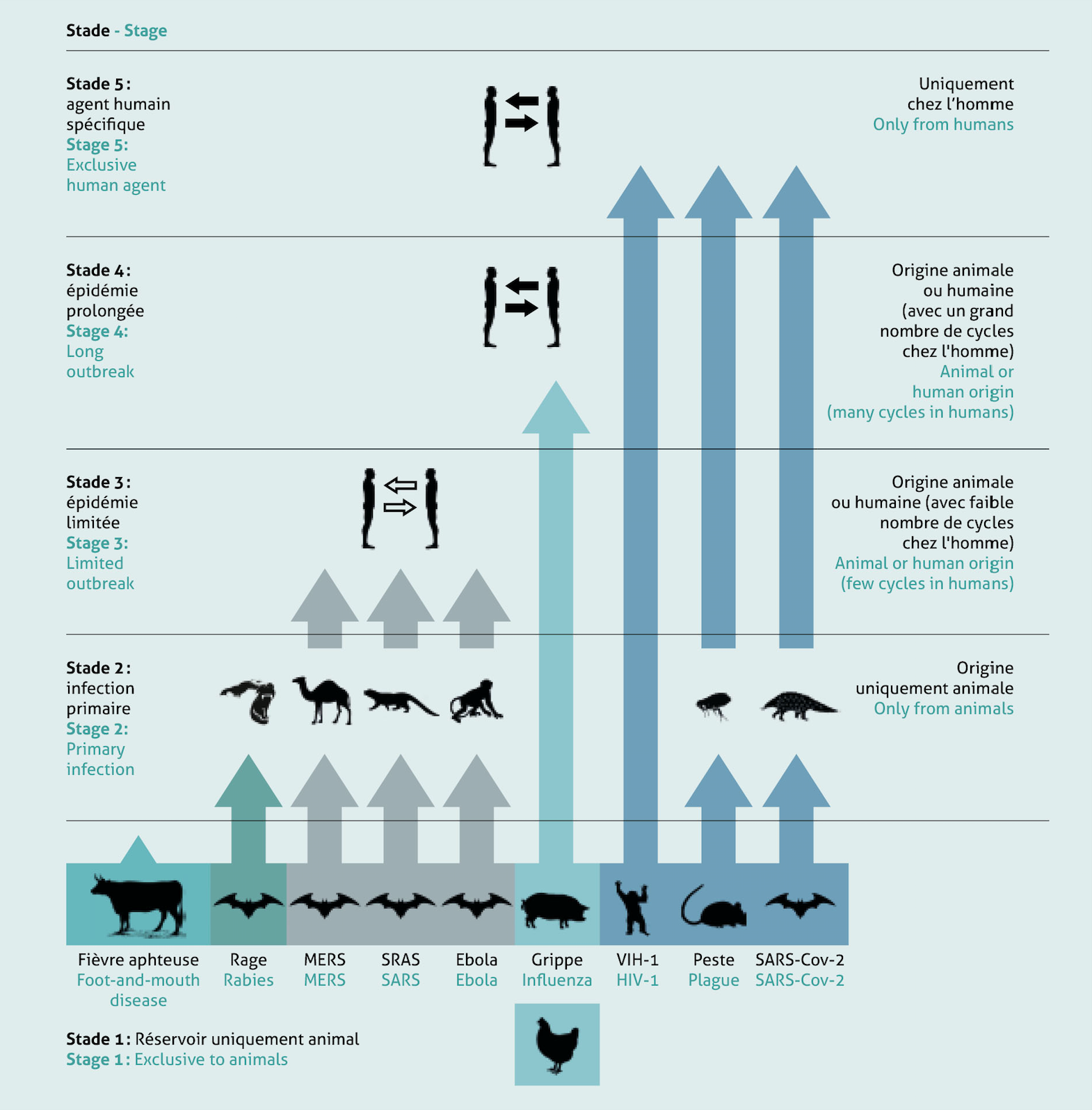
For an animal pathogen to become an effective pathogen in humans, it must be capable not only of infecting humans but also of maintaining long-term human-to-human transmission without the need for it to be reintroduced from the original host animal. Researchers[11]Nathan D. Wolfe, Claire Panosian Dunavan, Jared Diamond, “Origins of Major Human Infectious Diseases”, Nature, vol.447, 42, 2007, p.279-83, then Brian L. Pike et al., “The Origin and Prevention … Continue reading have identified five stages in the transformation of an animal pathogen into a human pathogen (Figure below). Stage 1 is characterised by animal microbes not present in humans under natural conditions, some of which will never be transmitted to humans (foot-and-mouth disease, rinderpest). When a pathogen evolves in such a way that it can be transmitted to humans under natural conditions but cannot sustain human-to-human transmission it enters Stage 2. Examples of such pathogens include the rabies virus and West Nile virus. The transition from Stage 2 to Stage 3 is defined by secondary transmission between humans. Stage 3 involves pathogens which undergo only a few cycles of secondary transmission between humans, such as the Ebola and Marburg viruses which periodically infect human hosts but fail to establish themselves in human populations. Stage 4 includes diseases such as influenza A and cholera which exist in animals but undergo long sequences of secondary transmission from human to human without the intervention of animal hosts. Stage 5, however, represents diseases that are exclusive to humans and includes pathogens such as human immunodeficiency virus (HIV), smallpox and tuberculosis[12]Ibid..
Our understanding of the emergence of human viruses is based on studies of the different types of reservoir and their contact with humans, mechanisms of viral genome variability, and many ecological, economic and social factors. The probability of an individual’s becoming infected increases with the abundance of the existing host and the frequency of “encounters” with the infectious agent, as well as the probability of transmission. This latter probability is also related to the characteristics of the microbe, such as its ability to overcome the host’s molecular barriers (e.g. its humoral and cellular defences) or the absence of cell membrane receptors essential for the entry of microbes into host cells. This explains why a given animal species can become the source of infections in humans; for example, despite the very low abundance of chimpanzees and their infrequent encounters with humans, they have been the source of established human diseases such as AIDS and perhaps hepatitis B because of their close phylogenetic relationship with humans – it is for this reason that primates, which account for only 0.5% of all vertebrate species, have contributed to around 20% of the major human diseases[13]Nathan D. Wolfe, Claire Panosian Dunavan, Jared Diamond, “Origins of Major Human Infectious Diseases…”, art. cit.. Conversely, even though they are phylogenetically very distant from humans, rodents, because of their abundance and proximity to humans, have transmitted major infections such as plague and typhus to them. The same can be said of domestic livestock because of their great abundance and daily contact with humans. On the other hand, it is known that bats do not transmit zoonoses to humans because of their phylogenetic remoteness and the rarity of their contact with them. With regard to bats, which constitute the main reservoir of viruses such as rabies, SARS, Ebola, and now Covid-19, infections in humans are mainly acquired from intermediate hosts that frequently encounter humans, e.g. dogs or foxes in the case of rabies, and wild animals sold as food in the case of SARS (civet) or Covid-19 (pangolin, although we do not yet know if it is involved). The rare cases of rabies transmitted directly by bats are due to the fact that the rabies infection alters bats’ behaviour, which means that they may bite humans and transmit the virus to them.
The ability to adapt to human beings was demonstrated during the 1997 outbreak of avian influenza in Hong Kong, which proved to be a formidable disease on poultry farms; it also affected eighteen people, six of whom died (30%). To stem this scourge, the Hong Kong authorities slaughtered 1.2 million chickens and 400,000 other birds, and closed the markets. The epidemiological investigation revealed that the human cases were the result of direct contact with poultry and demonstrated the absence of human-to-human transmission. The virus had indeed crossed the animal-human barrier several times but proved unable to adapt to humans to allow it to spread. The wholesale destruction of the virus reservoir, thus stopping the circulation of the avian influenza virus, certainly prevented it from evolving and perhaps from adapting to humans, which could then have caused an epidemic of dramatic proportions[14]Jean-François Saluzzo, Des hommes…, op. cit..
Figure – Some examples of the transmission of infectious agents from animals to humans and their adaptation, based on Wolfe et al. and Pike et al.[15]Nathan D. Wolfe, Claire Panosian Dunavan, Jared Diamond, “Origins of Major Human Infectious Diseases…”, art. cit., then Brian L. Pike et al., “The Origin…”, art. cit.
Criteria for assessing an epidemic
An epidemic reflects specific criteria of the microorganism, in particular its contagiousness and virulence, which affect how an infectious agent interacts with its host.
Contagiousness means the ability of an agent to cause infection in a susceptible host. One of the most important criteria for measuring the effectiveness of transmission is the basic reproduction rate of a virus or “R” value, which is the average number of new infections generated by an infected individual when the population is fully susceptible to the disease. The R value therefore depends not only on the infectious agent but also on the characteristics of the host population (e.g. number of contacts) in a given time period. It can range from R12 to R18 for measles or whooping cough, R2 to R5 for HIV, R2 to R4 for SARS, R2 to R3 for seasonal influenza and Covid-19, and R1 to R2 for Ebola. Depending on the actual R value, health monitoring institutes can determine whether or not a disease is likely to spread and cause an epidemic:
- R < 1 means that an infected person will infect up to one person. In this case, the number of new cases will fall rapidly and the presence of the disease in the population will fade;
- R = 1 means that an infected person will infect just one person. In this case, the number of new cases will increase on a regular basis without causing an epidemic;
- R > 1 means that an infected person will infect more than one person. In this case, the disease will spread through the population and may become an epidemic.
One of the most important criteria for measuring the effectiveness of transmission is the basic reproduction rate of a virus or ‘R’ value.
Virulence is the primary determinant of the severity of an epidemic and is measured by the number of serious cases or deaths. Infectious agents can be classified on the basis of their contagiousness and virulence: the Ebola virus, for example, has a very high virulence but low contagiousness which does not, however, prevent it from being a formidable predator.
| Covid-19
Coronaviruses belong to the Coronaviridae family of RNA viruses which are usually benign causing colds or influenza-like syndromes, but sometimes causing much more serious pulmonary tropism infections such as severe acute respiratory syndrome (SARS). The outer surface of the virus has a series of small, sharp proteins or spikes that give it the appearance of a crown (from the Latin corona), hence its name. These spikes play a fundamental role as they allow the virus to “cling” to host cells and enter them to inject their genetic material. Three coronaviruses responsible for SARS have been described: SARS-CoV-1 in 2002 in Guangdong, China; the Middle East Respiratory Syndrome MERS-CoV detected in Saudi Arabia in April 2012; and now SARS-CoV-2, also known as Covid-19. The latter seems to be highly transmissible and pathogenic. It appeared in November 2019 in Wuhan, China, and spread throughout the world. Genomic analysis has revealed that Covid-19 is phylogenetically linked to bat viruses. Bats are therefore highly likely to constitute the primary reservoir. The intermediate host and source of the transfer to humans is not known, although pangolins, a species of insectivorous mammal, are strongly suspected. Currently (3 June 2020), there are no clinically approved antiviral drugs or vaccines available for use against Covid-19. |
Factors conducive to epidemics
In addition to the microorganism’s own capabilities, various other factors may shape an infection in humans.
Overpopulation
The need to feed the world’s population in a sustainable manner is one of the main ecological and public health challenges of the 21st century. According to the United Nations, the number of people living on the planet is expected to rise from some 7.5 billion today to 9.7 billion by 2050, and could reach nearly 11 billion by 2100. In 2007, the world’s population became predominantly urban.
Plant and animal production will need to increase significantly to ensure that all humans have access to food, which will lead to increased use of water, pesticides, fertilisers and antibiotics, and even greater contact between humans and animals, both wild and domestic, all with consequences for the emergence and spread of infectious agents[16]Jason R. Rohr et al., “Emerging Human Infectious Diseases and the Links to Global Food Production”, Nat Sustain., vol. 2, 6, 2019, p.445-456.. Mortality rates from acute respiratory infections, diarrhoea, malaria and measles – diseases that, on average, kill at least one child every 30 seconds (1 million per year)[17]D. Webster, “Malaria Kills One Child Every 30 Seconds”, Journal of Public Health Policy, vol.22, 1, 2001, p.23-33. – are much higher among children who suffer from malnutrition[18]Pedro A. Sanchez, M.S. Swaminathan, “Hunger in Africa: The Link between Unhealthy People and Unhealthy Soils”, The Lancet, vol.365, 9457, 2005, p.442-444..
Displacement
Human mobility increased 1,000-fold between 1800 and 2000! The emergence of new pathogens is now facilitated by modern displacement, which increases the number of potential human victims. The Black Death of 1348, for example, took six months to reach Marseilles from its source in Kaffa , Crimea. In 2003, the SARS epidemic spread throughout the world in less than a week.
Global warming
Numerous studies refer to the role of climate change in the onset of infections. With 70% of the earth’s surface covered by water, global warming causes much more evaporation and, as a result, much more intense rainfall events, increasing the incidence of diarrhoeal infections worldwide. A 10% increase in diarrhoeal diseases is expected by 2030 and will mainly affect young children. Furthermore, high ambient temperatures accelerate the replication cycles of most food-borne and water-borne pathogens.
The El Niño phenomenon (the El Niño Southern Oscillation ) is a climate event that originates in the Pacific Ocean, but it has far-reaching consequences for the world’s climate. Globally, it is linked to the increased impact of natural disasters and is particularly associated with droughts and floods, as well as the transmission of infectious diseases, water-borne diseases and vector-borne diseases. El Niño is responsible for an increase in precipitation in East Africa and a decrease in precipitation in Southern Africa, West Africa and some parts of the Sahel. Due to the key role played by water supply in the transmission of cholera, a relationship between El Niño events and the incidence of cholera has been demonstrated[19]Sean M. Moore et al., “El Niño and the Shifting Geography of Cholera in Africa”, Proceedings of the National Academy of Sciences of the United States of America, vol.114, 17, 2017, … Continue reading.
Global warming is helping to spread mosquito-borne infectious diseases – such as West Nile fever, dengue fever, chikungunya, Zika, and also malaria – beyond their tropical homes. A comparison of mosquito maturation in forest huts and in deforested areas, where there was a difference of a few degrees in temperature, gave estimates of the percentage of insects that moved from larval to adult form that increased from 65% to 82%, while the period required for development fell from nine to eight days in warmer areas[20]P. Reiter, “Climate change and mosquito-borne disease”, Environmental health perspectives, vol.109, suppl. 1, 2001, p.141-161; Antonella Rossati, “Global Warming and Its Health Impact”, … Continue reading. Aedes albopictus, the tiger mosquito, for example, is becoming a serious threat in terms of the transmission of viral diseases such as chikungunya and dengue fever in Italy and southern France.
An increase in temperature accelerates the development cycle of ticks, their egg production, density and population distribution. In Europe, we are witnessing an increase in tick populations including Ixodes ricinus, the vector of viral infections such as tick-borne encephalitis and bacterial infections such as Lyme disease[21]Abdelghafar A. Alkishe, A. Townsend Peterson, Abdallah M. Samy, “Climate Change Influences on the Potential Geographic Distribution of the Disease Vector Tick Ixodes ricinus”, PLoS One, 5 … Continue reading.
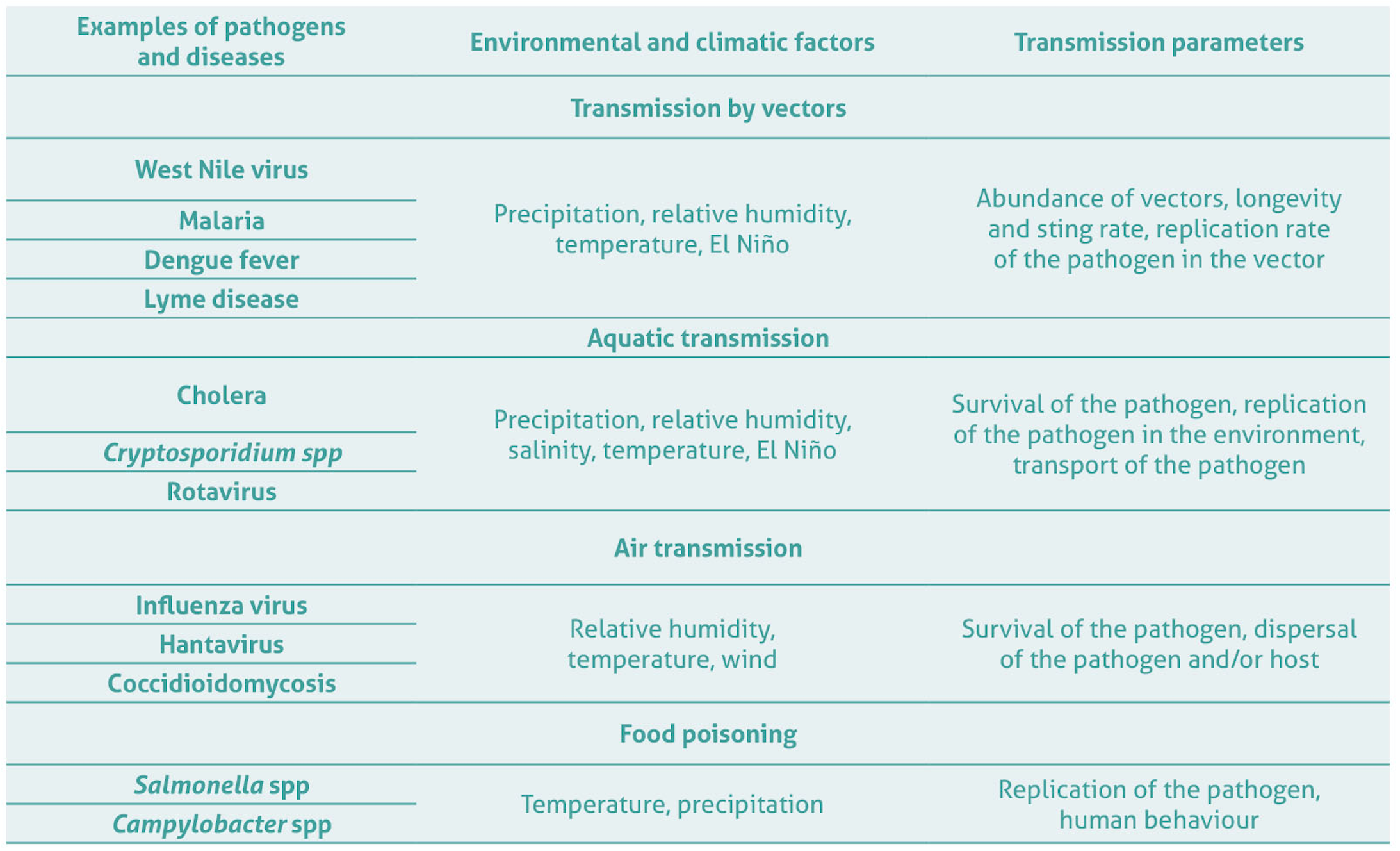
Table 2 – The relationship between global warming and infectious diseases, based on Cavicchioli et al.[22]Ricardo Cavicchioli et al., “Scientists’ Warning to Humanity: Microorganisms and Climate Change”, Nature reviews. Microbiology, vol.17, 9, 2019, p.569-586.
Deforestation
It is a well-established fact that clearing forests can lead to the transmission of zoonoses by increasing contact with wild animals. Increasing contact between human populations and forest pathogens to which they had never been exposed and the adaptation of these agents to humans have been demonstrated for HIV, yellow fever, dengue fever, chikungunya, Ebola, Nipah, SARS, rabies, malaria, Leishmaniasis and Lyme disease.
Epidemics caused by antibiotic-resistant bacteria
The extensive use of antibiotics by humans in the second half of the 20th century, their misuse, abusive prescriptions, and the heat- and humidity-induced deterioration of antibiotics in storage and when being transported have led to the extremely important phenomenon of bacterial resistance, particularly in developing countries where self-medication is very common. Furthermore, many drugs, including antibiotics, are counterfeited in these countries. The US Food and Drug Administration estimates that counterfeiting accounts for 10% of the pharmaceutical industry’s global turnover. Estimated at over €55 billion per year, the extent of the trafficking of counterfeit medicines varies from country to country. It can account for up to 60% of drugs in some developing countries, compared to 1% in industrialised countries with controlled, regulated distribution channels. The resulting antimicrobial resistance in bacteria is causing significant morbidity worldwide, with some estimates suggesting that attributable mortality could be as high as 10 million people per year by 2050 and become the leading cause of death worldwide[23]Carl Nathan, Otto Cars, “Antibiotic Resistance – Problems, Progress, and Prospects”, The New England Journal of Medicine vol. 371, 19, 2014, p.1761-1763; Jim O’Neill, “Tackling … Continue reading.
What about the post-Covid-19 world?
Man’s impact on ecosystems has gradually brought him into close contact with wild animals. In 2008, Kate Jones and her colleagues at University College London showed that 335 emerging infectious diseases were classified between 1940 and 2004, and that 60% of the emerging diseases described between 1980 and 2013 were of animal origin and of those, 70% had been transmitted by wild animals[24]Kate E. Jones et al., “Global Trends in Emerging Infectious Diseases”, Nature, vol.451, 7181, p.990-993.. For a little over a century, the world has witnessed the emergence of multiple infections, all of which are zoonoses: various strains of influenza (Spanish, Asian, Russian, Hong Kong, H5N1, H1N1 swine flu, etc.), AIDS, SARS, MERS, Lassa fever, Ebola, West Nile fever, Zika, chikungunya and Covid-19, not to mention the return of dengue fever, yellow fever, malaria, and even plague.
It seems highly predictable that other epidemics like the one currently affecting the planet will occur in the near future.
Given the staggering growth in the human population on the global level in recent decades, man’s inexorable footprint on nature (deforestation, loss of biodiversity, intensive livestock farming, uncontrolled antibiotic therapy, climate change, etc.) and the frequency with which human beings and goods move around, it seems highly predictable that other epidemics like the one currently affecting the planet will occur in the near future. We should therefore remember what the famous English ethologist and anthropologist Jane Goodall said about Covid-19: “If we don’t get that lesson from this pandemic, then maybe we never will”.
The author would like to thank François Renaud, Bernard Duchêne and Robert Abraham for their invaluable help in the preparation of this article.
Translated from the French by Derek Scoins
ISBN of the article (HTML) : 978-2-37704-666-9 |