





How did Canada, which has been particularly hard hit by the pandemic, organise itself? This collective of authors has undertaken a particularly instructive detailed review. We learn how non-governmental organisations, the Canadian Red Cross, provincial governments and the military came to support the medico-social teams.
Covid-19 presents huge challenges in terms of global public health, humanitarian emergency management, transparency and response time for a multitude of stakeholders at both the local and the international level. Since the beginning of the crisis, the state of health emergency in Canada has led to the temporary suspension of so-called non-essential economic activity, slowed down social activities, and revealed the presence of structural inequalities within the population. In terms of humanitarian aid, the Canadian State limited its actions to the national sphere in response to the crisis, with less attention being paid to international issues as a result. In Canada, when there proved to be too few professionals on the front lines or when these professionals were exhausted, the Canadian Red Cross (CRC) as well as the Canadian Armed Forces (CAF) were called in as reinforcements in order to assist the health systems in several Canadian provinces.
The Canadian government was forced to innovate by taking important decisions rapidly. In order to support the public health systems managed by the provinces and territories, Canada had to channel considerable financial resources and think up new programmes for public aid in concertation with the provinces to ease pausing the economy and making lockdown acceptable. Given the minority government situation, the Prime Minister was called on to create a collaborative work environment with other political parties and to encourage the civil service to work together with civil society organisations in order to facilitate the distribution of essential services for the population.
This article presents the ways in which Canada managed this exceptional situation at the national level (through authorities and non-governmental organisations and Save the Children), Affaires Mondiales Canada (AMC), and NGO networks including Coopération Canada and the Humanitarian Response Network (HRN). This enabled us to draw a varied portrait of the response to Covid-19, and to better understand the impact of the pandemic on the governance, resources, and programmes of these organisations.
The Canadian context
The Canadian health system is decentralised. Canada is effectively a confederation, which includes a federal government, ten provincial governments and three territorial governments. A constitution governs articulation between these levels. According to this constitution, the responsibility for health care and social services devolves to the provinces and territories. The federal government is also responsible for care for people in detention and for First Nations populations.
On 25 and 28 January 2020, the first isolated cases of Covid-19 were recorded in two provinces: Ontario and British Colombia[1]Daniel Blanchette Pelletier, « Comment s’est propagée la Covid-19 au Canada ? », Radio-Canada, mai 2020, … Continue reading. Emergency health measures were deployed from mid-March across the country. Since then, the pandemic has progressed in two waves. The first wave extended from mid-March to the end of June 2020. A period of calm, which lasted for a few months, led to a sharp decline in new cases, prior to a new surge in mid-September, when the number of new cases exploded and the death count began to climb rapidly[2]The second wave showed higher contamination rates amongst young people (and therefore less severe complications and deaths). The mortality rate (i.e. the relationship between the number of deaths and … Continue reading.
In qualitative terms, as of 3 October 2020, out of a population of roughly 38 million, Canada had 162,569 reported cases and 9,409 deaths attributed to Covid-19, with Quebec being by far the most affected province. Out of a population of 8.5 million, there were 76,273 cases and 5,857 deaths, approximatively 62% of all deaths related to the pandemic in the country. By comparison, in Ontario, the most populated province, with 14.5 million inhabitants, there were 2,927 deaths and 52,980 reported cases[3]See Gouvernement du Canada, Maladie à coronavirus (Covid-19) : Mise à jour sur l’éclosion – Situation actuelle, … Continue reading.
The pandemic profile during the first wave differed from that of the second wave. For the first wave, lockdown measures were rapidly announced towards the end of March, which limited community spreading. On the other hand, the virus severely affected private residences for the elderly and public housing centres providing long-term care for seniors, where the death toll was highest[4]85% of deaths occurred in these living environments. See Comparaisons Santé : Québec/Canada/OCDE, « Mortalité par Covid-19 au Québec : comparaisons nord-américaines et internationales », … Continue reading.
During the second wave, the protection measures implemented by organisations and institutions that had been victims of Covid-19 were effective to the point of avoiding the development of major clusters. Propagation essentially took place in communities amongst younger people – especially amongst 20-29-year-olds, who represented 25% of all new cases in Quebec[5]Mélanie Meloche-Holubowski, « Les jeunes au cœur des nouvelles éclosions de Covid-19 », Radio-Canada, 9 septembre 2020, … Continue reading. The spectre of a second lockdown and reduction of the economy to essential activities forced governments and public health authorities to adapt quickly by developing new measures and new forms of action, such as strictly limiting travel and private gatherings[6]Measures varied from one province to another. For example, Quebec had a colour system for alerts; Ontario implemented specific measures relative to education..
The actors of the response
The Canadian health system: structural limitations propitious to the development of the pandemic
In terms of vulnerability analysis, the reflex would be to assume that a strong State[7]According to the Index of Fragile States, developed by Fund for Peace (2019), Canada is considered to be an efficient, or strong State. would be able to offer uniform coverage of goods and services at the national level. In fact, the degree of resilience within the national space is not uniform[8]Diane Alalouf-Hall et Jean-Marc Fontan, « Gestion des catastrophes naturelles en sol québécois : rendre socialement et écologiquement responsables les processus de développement des … Continue reading. In the context of Covid-19, the regions in the affected countries did not present a similar capacity for territorial resilience. In Canada, certain regions with low levels of socio-territorial capital[9]“This capacity of the local environment to create ‘surplus social value’ from new organisational and institutional arrangements is an element of socio-territorial capital” in Jean-Marc Fontan … Continue reading were significantly disadvantaged in the face of the crisis, which led to a more virulent propagation of the virus in certain communities or in certain geographical areas.
The Canadian health system is based on five fundamental principles (Canada Health Act, 1984): universality (all citizens are covered), comprehensiveness (all essential medical and hospital services are covered), portability (the cover is valid throughout all of the provinces and territories), public administration (the provincial and territorial health care insurance plans must be managed by a public agency on a not-for-profit basis), and accessibility (reducing financial barriers that impede access to health care)[10]Canada Health Act: https://sencanada.ca/content/sen/committee/372/soci/rep/repoct02vol6part7-f.htm.
The Canadian public health system as we know it today was first developed in 1947[11]Gouvernement du Canada, Le système des soins de santé du Canada, https://www.canada.ca/fr/sante-canada/services/systeme-soins-sante/rapports-publications/regime-soins-sante/canada.html. The provinces and territories are the contractors in terms of health and public services. They are responsible for maintaining the free, public, and universal character of their health system.
In Quebec, given the ageing population, the overrepresentation of seniors amongst the victims of the pandemic[12]Until late April 2020, more than 80% of deaths linked to Covid-19 in Quebec occurred in residential and long-term care centres. during the first wave gave the impression that the disease mainly affected elderly people. And yet, alongside vulnerabilities linked to age and states of health (chronic illnesses), the pandemic showed that it severely affected those that society had made vulnerable and those who daily provided their care[13]Estelle Carde, « La Covid-19 creuse les inégalités d’aujourd’hui, mais aussi celles de demain », The Conversation, 27 mai 2020, … Continue reading. In Quebec, more than 40% of over-85-year-olds live in a private or public housing establishment. This is the highest rate in Canada[14]Fabien Deglise, « Pourquoi la Covid-19 frappe-t-elle plus le Québec ? », Le Devoir, 30 avril 2020, … Continue reading. The propagation of Covid-19 can be explained not so much in relation to the seniors’ age, but rather in relation to the way in which seniors and ageing are treated in Quebec. Two administrative inquiries commissioned by the Ministry of Health (Autumn 2020) revealed structural and organisational failures which contributed to the propagation of the virus in the establishments for long-term health care: clinical protocols that were rarely up to date, missing, defective or ill-adapted equipment, and, above all, a severe shortage of staff due to a lack of financial resources[15]These problems were documented by the Ministry of Health and Social Services: « Rapport d’enquête sur les événements survenus dans le cadre de la pandémie de la Covid-19 au CHSLD Herron », … Continue reading.
The deployment of military actors in long-term health care establishments
Faced with this uncontrollable spike in contaminations and deaths in several long-term care centres in Quebec and Ontario, the Prime Ministers of the two provinces turned to the federal government to ask for emergency aid. The call was answered, and the government decided that Operation LASER[16]Operation LASER refers to the global CAF response to reduce the national repercussions of the pandemic. In this article, we focused solely on the support mission within long-term care centres. For … Continue reading would deploy military personnel in the most severely affected long-term care centres.
In Quebec, a first contingent of 1,000 members of the CAF was deployed in twenty residential and long-term care centres in the Greater Montreal area. 670 military personnel from amongst this contingent had prior medical training, whereas the others were there to provide logistical support for the centres’ day-to-day operations[17]Louis-Samuel Perron, « CHSLD : plus de 1 000 militaires déployés sur le terrain », La Presse, 7 mai 2020, … Continue reading. Several days after this deployment, a second contingent of 350 military personnel arrived in five other long-term care centres, where the situation was judged to be critical. In Ontario, the Prime Minister obtained 250 military personnel being posted from 28 April. They were deployed in groups of fifty in five long-term care centres in the Greater Toronto area.
Overall, as part of this intervention, the CAF were present in fifty-four long-term care centres (forty-seven in Quebec and seven in Ontario). Provincial governments asked the federal government to extend the military presence until the end of June, at which point the CAF were gradually replaced by CRC personnel. Over the course of this operation, thirty-nine military personnel contracted Covid-19 – twenty-four in Quebec and fifteen in Ontario[18]La Presse canadienne, « 39 militaires infectés dans des CHSLD du Québec et de l’Ontario », Radio-Canada, 26 mai 2020, … Continue reading. None of the military personnel infections by Covid-19 resulted in deaths.
It is important to recall the exceptional character of army participation in supporting Canadian public authorities for service provision for health needs. Normally, this kind of intervention is carried out outside of the country, in a context of international solidarity (Canadian Disaster Response Team), and in response to large-scale humanitarian situations (such as the tsunami in 2004, Haiti in 2010, or in 2014 as part of the fight against the Ebola virus in West Africa[19]Government of Canada, Canada’s Response to the Ebola Outbreak in West Africa, https://www.canada.ca/en/news/archive/2014/10/canada-response-ebola-outbreak-west-africa.html). Exceptionally, the army has intervened on Canadian soil to assist with national security issues (October Crisis, Quebec, 1970), or to assist the population in the wake of natural disasters[20]According to La Presse canadienne, there have been forty-two CAF interventions following natural disasters on Canadian soil – twelve times between 1996 and 2006, twenty times between 2007 and … Continue reading. But in terms of health care, this was the first time that military personnel had been directly mobilised to intervene on Canadian soil.
The intervention by the CAF in response to the pandemic was intended to provide logistical assistance, primarily for routine operations that needed to be carried out in order to ensure the proper functioning of the long-term care centres. CAF members carried out different tasks according to the variable needs of each establishment: meal preparation, hygiene for the elderly, and site disinfection. To fulfil these roles, those military personnel who did not have prior medical training followed a short training course given by CRC professionals[21]Incidentally, in Quebec alone, the CRC trained some 9,600 people in the use of PPE and prevention- and infection-control., which enabled them, amongst other things, to learn to use personal protective equipment (PPE) effectively, and to administer certain basic services to the beneficiaries.
In terms of health care, this was the first time that military personnel had been directly mobilised to intervene on Canadian soil.
The CAF also acted as whistle-blowers, publishing two critical reports which were delivered to the governments of Ontario and Quebec. The Ontario report[22]SCRIBD, « Rapport (en anglais) des Forces armées canadiennes sur les cinq centres de soins de longue durée dans la région de Toronto », … Continue reading (May 2020) reported the presence of cockroaches, mould in the distributed food, the use of out-of-date medicines, and the reuse of non-decontaminated equipment. It also mentioned that bedridden seniors were left in soiled bedding, leading to several of them being subjected to bedsores[23]Marie Vastel et Magdaline Boutros, « L’armée décrit l’horreur dans les CHSLD en Ontario », Le Devoir, 27 mai 2020, … Continue reading. Military personnel reported intimidation on behalf of the personnel in the centres. The Quebec report[24]« Rapport FAC – Observations », 2020, https://cdn-contenu.quebec.ca/cdn-contenu/sante/documents/Problemes_de_sante/Covid-19/Rapport_FAC/Observation_FAC_CHSLD.pdf?1590587216 was not so shocking. It highlighted recurring problems in the long-term care centres, such as laxity in terms of surveillance and monitoring on behalf of centre directors, lack of discipline in certain centres with regard to the use of PPE, and finally, the critical lack of assistants for the beneficiaries.
A “nationalised” humanitarian actor
Based on its experience in the fight against epidemics (cholera, Ebola…) in seventeen countries, the CRC quickly intervened in Canada by offering support to overwhelmed consular services for citizen repatriation. It set up a field hospital at the military base at Trenton and reinforcements for the one in Cornwall to support Canadians in quarantine returning from overseas. The CRC took rapid action in a dozen sites throughout the country, providing support for more than 3,000 Canadians. Two other field hospitals were set up in Montreal and Vancouver to assist hospitals that were overwhelmed. The organisation also provided support for 200 indigenous communities thanks to its helpline.
The central role of the CRC was reflected in the direct support provided to the long-term care centres in Ontario and Quebec, where there was a chronic lack of personnel. 900 members of the CRC were directly involved with the long-term care centres to support health professionals. The CRC response, from the first wave to the present day, involved financing of 100 million Canadian dollars, which was granted by the federal government.
Covid-19 has highlighted the importance of redefining the organisation’s role on Canadian soil. Even before the pandemic, the CRC had been negotiating to reinforce its auxiliary role alongside public services, with a view to meeting public health protection needs in the country[25]In Canada, aside from the CAF, there is no civil protection mechanism with enough resources – especially human resources – to intervene in the event of large-scale disasters.. The CRC has been responding to large-scale crises for several years, but its private funding has not always reflected this. Incidentally, at the beginning of October 2020, it was announced that the federal government was planning to officially request that the CRC provide support in areas that had been severely affected by the pandemic, by means, amongst others, of logistical support in testing centres and in senior accommodation centres[26]See Catharine Tunney, “Federal government offering Red Cross support to Covid-19 hotspots: sources”, CBC News, 1 October 2020, … Continue reading.
The CRC’s national response to Covid-19 consolidated the organisation’s international response and increased its impact and visibility thanks to a demonstration of its skills, resources, and awareness-raising capabilities. The CRC also set up prevention and infection-control teams to support 110 long-term care centres. In under 24 hours, each team was able to evaluate a long-term care centre and compile a report providing recommendations, before subsequently accompanying the centres in the implementation of these recommendations. This way of working, which was greatly appreciated by the long-term care centres, had the advantage of remaining confidential between the CRC and the centres. Throughout their interventions, CRC teams developed a standard approach for the centres and a bank of recommendations which will be useful in the future.
More than 70% of unearmarked humanitarian funding was therefore allocated to health and food aid organisations.
Other Canadian NGOs responded to the health crisis in different ways. For example, MSF shared its available personnel with the CRC. The organisation, which had never been operational in Canada, seriously considered opening a 400-bed centre for marginalised groups (homeless, refugees, indigenous people, etc) in Toronto. The centre was never built, since the authorities preferred to invest in a crisis management model that involved putting vulnerable people up in hotels instead of sending them to the centre proposed by MSF. The organisation was nevertheless able to offer support for the evaluation of centres for homeless people in order to ensure the respect of public health measures, and to offer support to indigenous communities. In the same way, MdM continued its work with precarious populations via mobile clinics in Montreal and Victoria. MdM quickly developed telemedicine facilities thanks to support from a hundred volunteer doctors, and nurses from mobile teams went into the streets with their rucksacks and PPE to help people in need. The organisation continued its prevention work, providing equipment to inject drugs and raising awareness amongst public authorities. For its part, IR worked with local partners to raise awareness, provide support for quarantine centres, supply hygiene kits, etc.
The Canadian Red Cross (CRC) creates a new humanitarian “reserve workforce” to support the Covid-19 responseAt the end of October 2020, with the rise of Covid-19, the Government of Canada has established a partnership with the CRC to ensure the preparation and response to the second wave of the pandemic and to use the organisation’s experience and expertise to support screening, immunisation, outbreak crisis management, long-term care, contact tracing and more, if needed. This requires the development of new working methods to make its humanitarian force even more stable and quick to mobilise, with a new category of personnel: the “reservists”. What will distinguish “reserve workforce” positions from regular volunteer positions is the commitment that reservists must make as to their availability. Those selected will be deployed at very short notice (usually within 24-48 hours). The reserve force will allow the CRC to begin new operations quickly. To fill this new workforce, the CRC will post offers for full-time, casual and volunteer positions. |
The Canadian humanitarian response at the international level
The CRC was active in China as early as December 2019. Thanks to close contact with people in the country, it engaged in an exchange of good practices, facilitated logistics and proceeded to send equipment (sixteen tonnes of PPE to begin with[27]An official agreement planned a five-fold return of assistance in the case of need in Canada. Recent history has shown that this “investment” has been profitable for Canada since China supported … Continue reading). A first contribution of 2 million dollars was allocated to the World Health Organization (WHO) with a view to helping vulnerable countries to prepare for the fight against Covid-19.
Soon after Canada closed its borders in March 2020, the Canadian government announced a first funding initiative (50 million), intended to help the most vulnerable countries to prepare for the fight against Covid-19 by reinforcing surveillance and infection-prevention systems, supplying water and hygiene and sanitation services, emergency healthcare and psychosocial support. The Canadian response to support global efforts in the fight against the pandemic was consolidated in June with the announcement of “unearmarked” contributions, which were almost exclusively channelled through the multilateral humanitarian system, to the tune of nearly 170 million dollars.
More than 70% of unearmarked humanitarian funding was therefore allocated to health and food aid organisations. In total, the Canadian government committed more than 850 million dollars in research and development, both on the national level and in international support in the context of the financing campaign of the “global response to coronavirus”. This led Coopération Canada to state in June 2020 that with this new funding, “Canada’s contribution to the global response to the pandemic represents less than 0.25% of the federal government’s spending on the national level”. For the Canadian Humanitarian Response Network, “all the money went to the global system”, and we do not yet know whether there was a trickle-down effect as a result of funding that might have been allocated to Canadian agencies by certain UN agencies.[28].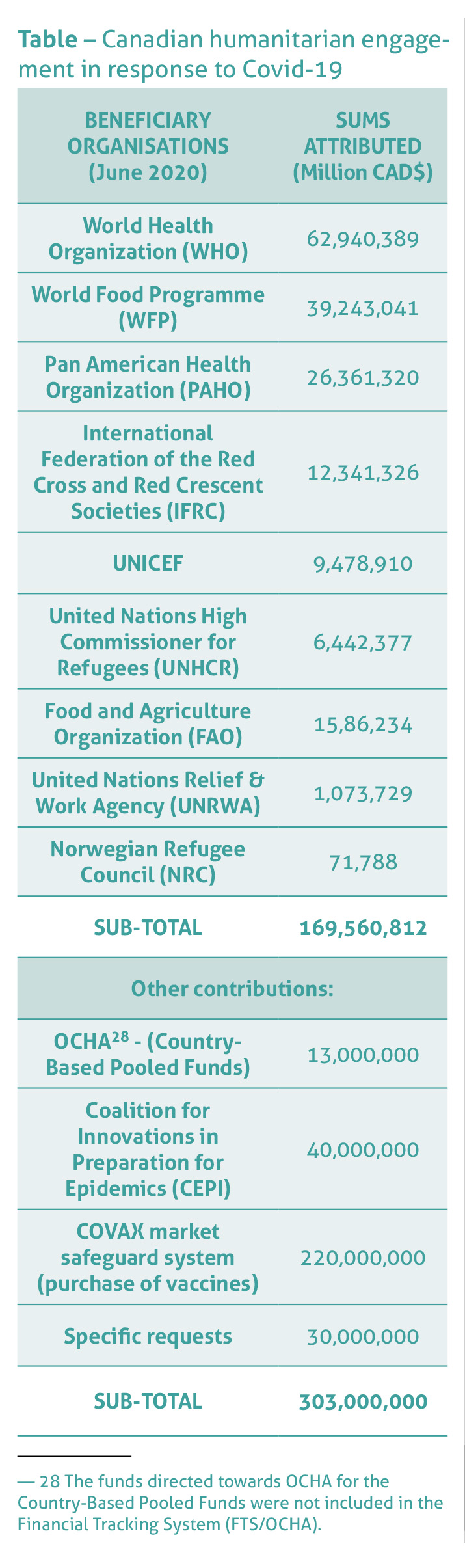
Canadian humanitarian NGOs did not benefit from specific funding from the AMC to take part in the fight against Covid-19 either. They were invited to continue their usual engagements, pursuing the same goals and humanitarian activities funded by AMC before the crisis. No call for contributions was launched to reinforce their programmed intervention at the international level. The organisations that were active on the front lines of the pandemic used their own resources in association with their local partners (like Développement et Paix) or their international networks (like MdM or IR). The HRN did not launch any specific call for the AMC to build a common response between humanitarian agencies and the Canadian government. It expressed concern that, in the absence of targeted contributions, certain agencies would not be able to continue to work in a sustainable way, or may be forced to limit their programmes. Humanitarian organisations are conscious of the fact that the long-term effects of the crisis may significantly affect refugees and displaced persons in several areas throughout the world, but they lack the visibility to know how to manage this.
A new response is being prepared. At the end of September, at the 75th session of the United Nations General Assembly, the Prime Minister of Canada announced an additional contribution of 400 million dollars to support the recovery and resilience of developing countries, as well as to respond to the short-term humanitarian needs linked to the pandemic[29]Justin Trudeau, Prime Minister of Canada, “Prime Minister co-chairs high-level meeting to address economic devastation caused by COVID‑19 and announces new funding to fight the pandemic”, … Continue reading.
The impact of Covid-19 on Canadian humanitarian aid
Our interviews revealed that the impact of the pandemic on Canadian NGOs’ human resources, finances and programmes was variable. The organisations that employed volunteers and international delegates repatriated some or all of their Canadian employees. In terms of fundraising and management, certain organisations were able to play their cards right by adopting a flexible approach. For example, against all odds, IR was able to adapt its fundraising methods and succeeded in generating more income in the spring (Ramadan period) than over the same period the year before. For some organisations, the decrease in private revenue (events, collections during ceremonies in places of worship, which were closed) had devastating effects on their finances, thereby endangering their very existence. Covid-19 will undoubtedly trigger significant changes in fundraising techniques. Some organisations laid off human resources or asked for government help in order to survive. Others came to an agreement with their personnel, making them work less in order to reduce salary costs for a certain number of months.
Some international NGOs also decided to put their national offices in dormant mode or to transfer responsibilities to the local level[30]This trend towards localisation happened by necessity, but its sustainability remains in question for a number of actors.. For most, new initiatives were suspended, with the exception of sudden emergencies such as in the wake of the explosion in Beirut in August. Current projects and programmes are continuing with pre-existing budgets, with interventions being adapted to public health measures. New project proposals will depend on government announcements and on the development of the pandemic.
A study from the Université Guelph[31]Andrea Paras et al., The impact of the Covid-19 Pandemic on Canada’s Foreign Aid Sector, 2020, University of Guelph, https://gids.uoguelph.ca/system/files/Covid19%20Report_Final_2.pdf confirms a number of our observations. The first impact of the epidemic reported by the team is the decrease in funding: 60.1% of organisations reported a decrease in funding since March 2020 and the average amount of this decrease was 26.4%. Small and medium-sized organisations have been worst affected, since their portfolios are less diversified, and they tend to be financed mainly by private donations. Although the pandemic has exacerbated pre-existing problems in developing countries, a number of NGO programmes have been suspended (especially in the fields of education and gender equality). The study reported optimism in the sector with regard to the acceleration of the reinforcement of local actors (localisation) but recalled the administrative difficulties and financial conditions which remain an obstacle to its implementation.
Covid-19 will undoubtedly trigger significant changes in fundraising techniques.
In summary, the impact on NGOs depends largely on the kind of organisation and the model of financing. In the long-term, certain organisations will no doubt be led to review their ways of working and to call into question some of their policies and practices.
Possible opportunities
As a result of our reflexive approach, we observed that the Canadian response to the threat represented by the Covid-19 pandemic revealed a number of opportunities.
Firstly, this is the most significant health crisis since the HIV-AIDS epidemic. Its significance is due less to the number of deaths, which is relatively low compared to AIDS, than to the impact of the disease on socioeconomic activities (recession) and on the most modern health systems in the world (leading to overcrowding and dysfunctions). The incidence of this disease is socioeconomic (impact on global and national economic growth), socio-sanitary (overwhelming of health systems and social services), and geopolitical, due to the trend of brutal national withdrawal (repatriation of humanitarian resources and closure of borders), more than it is sociodemographic (mortality rate linked to Covid-19).
Secondly, and linked to the first element, the threat of this pandemic resides in the fact that it acts on two of Canada’s weaknesses. The first is socioeconomic. Covid-19 affects people in vulnerable situations: the elderly, the destitute, people suffering from chronic diseases, medical personnel exposed to the disease, etc. The second weakness is institutional. Covid-19 benefited from structural weaknesses in health systems in order to spread. The pandemic was exacerbated by social inequalities (greater exposure amongst marginalised and destitute groups), and by institutional weaknesses in terms of public policy (shortcomings in policies on ageing) and the severe lack of resources in the health systems and social services.
Thirdly, the Canadian State’s response to the first wave of the pandemic was firm, albeit chaotic at times. It consisted in:
- protecting the population: border closures, lockdown measures;
- transferring financial resources to maintain the Canadian economic system afloat: universal income for employed people, measures to help businesses, special programmes using emergency funds;
- mobilising key organisations: in terms of national security (the armed forces), humanitarian aid (CRC), and emergency services for the population (support for the community sector to provide basic services: food, shelter…)
For the second wave, to date, the response has been both firm and level-headed: guaranteeing a maximum of economic activities whilst maintaining a maximum of preventive measures and a relatively decent level of timely emergency measures.
Fourthly, for Canadian humanitarian organisations, the response was carried out on several fronts, whilst cumulating economic constraints. We were able to observe the retreat of a percentage of humanitarian personnel for reasons of employee security. This choice effectively placed local organisations on the front lines. Moreover, significant changes are to be expected with regard to fundraising techniques.
Covid-19 benefited from structural weaknesses in health systems in order to spread.
Whilst waiting for a vaccine to be developed, the different Canadian responses to this pandemic have paved the way for important transformations. Covid-19 has represented an opportunity to proceed with major changes in ways of living (lockdown and hygiene habits), ways of working (working from home), and State capacities to mobilise a diversity of resources (timely emergency measures, the Canadian army, CRC, civil society organisations…), but also for humanitarian organisations to rethink their ways of working abroad (localisation, transfer of resources, financing…).
Overall, we are far from having exhausted the potential of the forced opportunities presented by Covid-19, and we are also far from having implemented sufficient measures to contain its threat.
Translated from the French by Juliet Powys
ISBN of the article (HTML) : 978-2-37704-749-9 |



